Reviews
Cataract surgery in Houston: Cost, insurance, and the decisions people avoid until the last minute

Cataract surgery in Houston is a medical search, but it is also a planning search. People who make that search are often trying to solve two problems at once: they want to see clearly again, and they want straight answers about what is covered, what is optional, and what the trade-offs look like. Research on shared decision-making in intraocular lens selection shows that cost management, preparation, and patient participation are part of decision quality, not side issues. [1]
Cataract surgery cost is not one number because the decision is rarely just about removing a cataract. It also includes choices about lens goals, tolerance for glasses, ocular findings that may limit eligibility for certain options, and the patient’s own priorities. That is why the cost conversation should happen early: when patients understand the options, they make better-aligned decisions and are more satisfied with the result. A useful way to frame it is this: cataract surgery restores clarity, but planning determines how you live with that clarity. [1]
Start with the decision you actually need to make
The first decision is not whether the most advanced option sounds appealing. The first decision is what outcome matters most in daily life. Shared decision-making research in cataract patients shows that preparation and participation are closely linked to satisfaction with the decision, which means the best consultation is usually the one that begins with priorities, constraints, and lifestyle rather than marketing language. [1]
Why upgrades exist (and who benefits most)
Upgrades exist because some patients want to reduce dependence on glasses, especially for near vision or astigmatism correction. But candidacy is individualized. Patients with concurrent corneal disease may sometimes still be candidates for premium IOLs, yet the decision depends on whether the cornea can be accurately evaluated and, in some cases, treated first. In other words, an upgrade is not automatically the “better” choice. The right upgrade is the one your eye can support. [5]
The trade-offs that matter more than marketing
Trade-offs matter more than slogans. Outcomes depend not only on lens technology but also on measurement quality, ocular surface stability, and expectation management. Jai G. Parekh emphasized the importance of ocular surface health before cataract and refractive surgery, noting that dry eye and related surface disease are common and can affect preoperative measurements and the quality of the visual result. [3]
Patients also do not always feel equally informed about every part of the decision. In a 2014 patient survey published in Clinical Ophthalmology, about 85% of respondents who had undergone cataract surgery felt well educated about the procedure, but only 75% felt they understood their lens and vision options. That gap matters because satisfaction is often shaped less by the surgery itself than by whether patients understood the trade-offs beforehand. In cataract surgery, trade-offs decide satisfaction more than slogans do. [4]
Financing questions are normal questions
Financing is part of access, and access is part of care. Patients often avoid cost discussions because money feels personal, but a vague cost discussion can lead to a weak decision. The shared decision-making study explicitly places cost management inside the IOL selection process, which supports treating financial clarity as a clinical communication task rather than an awkward afterthought. A cost conversation is a trust conversation. [1]
How to compare clinics without guessing
Comparing clinics becomes easier when you compare processes instead of adjectives. One meaningful question is whether the practice uses preoperative retinal OCT. OCT before cataract surgery can detect vision-limiting macular pathology that may be missed on standard examination and can reduce postoperative “visual surprises,” which directly affects counseling and expectation setting. Compare workflows, not adjectives. [2]
A second useful question is how the clinic handles the ocular surface before measurements are finalized. Dry eye, blepharitis, and other forms of ocular surface disease can make measurements less reliable and can undermine the quality of the outcome if they are not addressed first. A third question is how the surgeon explains lens candidacy when corneal irregularity or other ocular factors are present. These are practical markers of decision quality because they reveal whether the clinic is matching technology to the eye in front of them. [3][5]
What to ask at your consult
A strong consult usually comes down to a few direct questions:
- What is medically necessary, and what is elective?
- How do you decide whether I am a candidate for a premium lens?
- Do you check for retinal problems with OCT before surgery?
- Do you treat dry eye or other ocular surface disease before final measurements?
- How do you counsel patients about glasses after surgery?
Those questions are not difficult. They are the questions that prevent last-minute regret. [1][2][3][5]
The bottom line that helps you decide
Cataract surgery is not just a procedure decision. It is a planning decision. Cost transparency reduces confusion. Better preoperative evaluation reduces surprises. Better education about lens options reduces regret. And a more individualized conversation improves the odds that the result will fit the patient’s actual life, not just the brochure version of it. [1][2][3][4][5]
References
[1] Jingyao Dai, Yiting Hua, Yijie Chen, Jiali Huang, Xiaoxian Zhang, Yiwen Sun, Chen Chen, Yanyan Chen, and Kaijing Zhou, “Current Status of Shared Decision-Making in Intraocular Lens Selection for Cataract Surgery: A Cross-Sectional Study,” June 24, 2024.
[2] Cheryl Guttman Krader, “Pre-cataract surgery OCT means happier patient outcomes,” November 15, 2020.
[3] David Hutton and Jai G. Parekh, “The importance of ocular health prior to cataract and refractive surgery,” February 28, 2023.
[4] Bonnie An Henderson, Kerry Solomon, Samuel Masket, Richard Potvin, Edward J. Holland, Robert Cionni, and Helga Sandoval, “A survey of potential and previous cataract-surgery patients: what the ophthalmologist should know,” August 25, 2014.
[5] Ophthalmology Times, “Premium IOLs in corneal disease an individualized decision,” May 5, 2017.


Major 7.8 earthquake strikes Philippines, tsunami threat issued

2 killed after U.S.-registered private jet crashes in Dominican Republic

9 injured in Kansas City shooting

Actor James Handy killed by girlfriend’s son at Los Angeles home
-

 World1 week ago
World1 week agoDutch police review arrest after pregnant woman thrown to ground in viral video
-

 World1 week ago
World1 week agoU.S. citizen killed in shootout near Cabo tourist area in Mexico
-

 US News1 week ago
US News1 week ago3 Latvian climbers killed in fall on Denali in Alaska; others injured
-

 Legal1 week ago
Legal1 week ago2 officers, police K-9 injured in Virginia shooting
-
 US News1 week ago
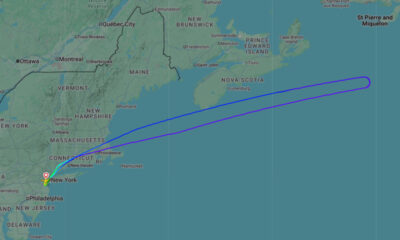
US News1 week agoUnited flight turns around over Atlantic after Bluetooth device named BOMB
-

 Legal6 days ago
Legal6 days ago3 killed, officer wounded in shooting in Sandy, Oregon
-

 Legal6 days ago
Legal6 days ago1 killed, 1 seriously injured in shooting near clinic in Saskatchewan, Canada
-

 Legal4 days ago
Legal4 days agoMississippi deputy shot during standoff in Simpson County